
Tidbits #19: Raynaud's Phenomenon
Welcome to Friday Tidbits. This is a short email with morsels of information to help you tweak your life and health for optimum longevity and healthy ageing. This newsletter is free every 2 weeks.

White Fingers in Cold Weather - is it Raynaud’s Phenomenon?
I manage to get to the beach most mornings after exercise. Quite a few small groups meet between 6am and 7:30am and brave the cold ocean - all year. Yes, even in winter. We are quite lucky, the winter ocean is mostly 16C (or 61F). On a few occasions it will dip to 11C (or 52F).
We stay in the water between 5 and 20 minutes, depending on conditions. It is a daily ritual for many. And we miss it if we can’t get there for extended periods. Don’t get me wrong, on cold and windy winter mornings it is a mental challenge in resilience to peel off layers of warm clothes and walk into the ocean. The 1st minute is the hardest.
Over the years, we all got to know one another. We may not know the names but the faces become familiar. There is a social phenomenon regarding enduring difficult situations as a group. Something like “those who suffer together will be firm friends”. But let me not get side-tracked.
Terry, is one of my fellow winter cold plungers. Last week she showed me her very white and very painful finger tips. She has a condition called Raynaud’s Phenomenon.
I have quite a few friends with this condition - it occurs in 5% of the population (1).

Figure from Herrick AL, Wigley FM. Raynaud's phenomenon. Best Practice & Research Clinical Rheumatology. 2020
What is Raynaud’s Phenomenon
In an abnormal response to cold temperature, smaller arteries spasm (vasospasm) and restrict blood flow to parts of the body, typically the fingers and toes. Other areas that can be affected include the nose, ears, knees and nipples. The skin of the affected area first turns white due to the lack of (warm) blood and can even become blue if it lasts for a long time and oxygen levels fall below normal. In very severe cases, it can lead to tissue injury. When blood flow returns (this is called repurfusion) the skin becomes bright red and it can be very painful.
Raynaud’s is a condition of poor blood circulation to an area.
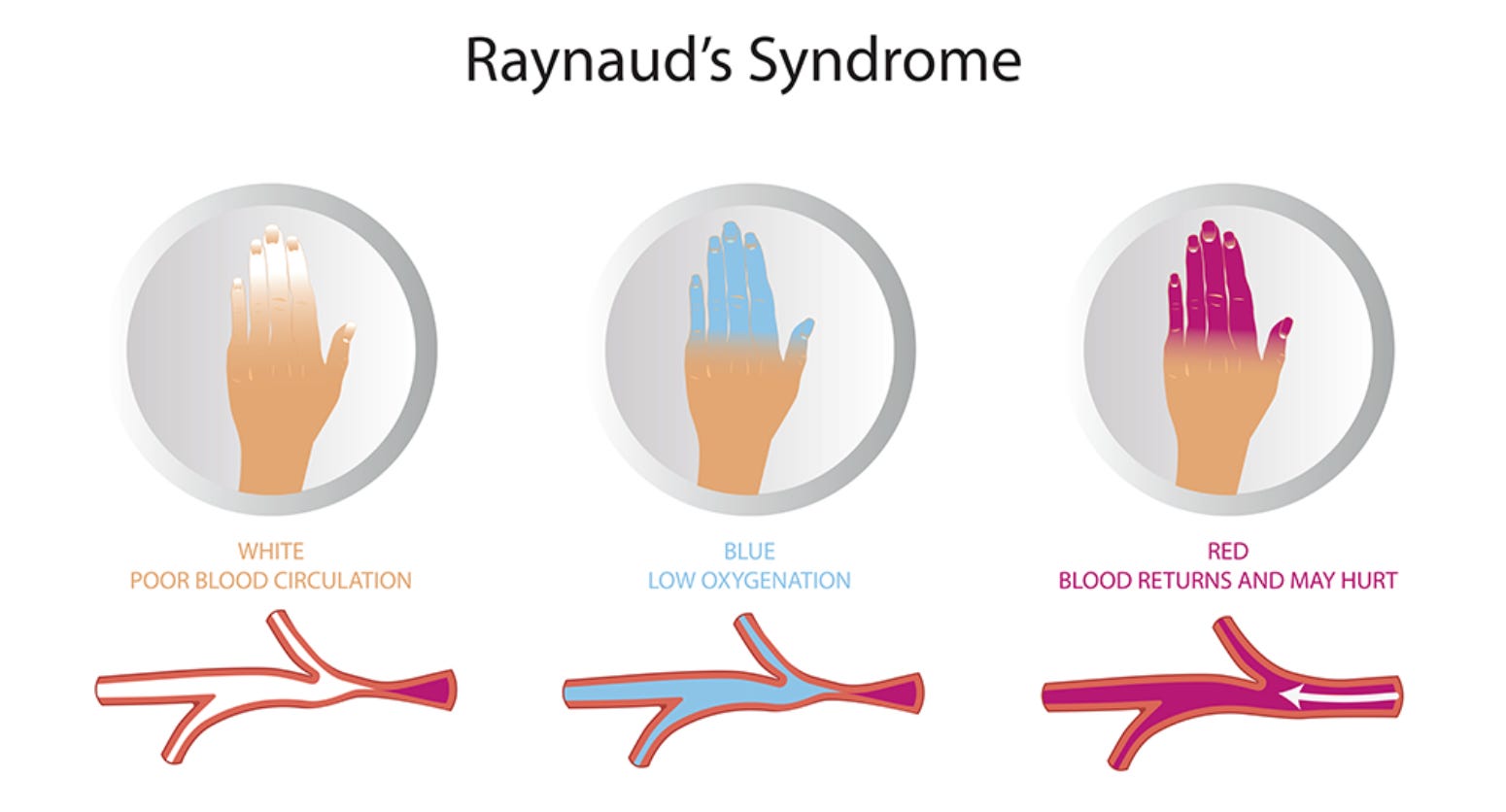
Figure from viasonix.com
Raynaud’s was first described in 1862 by a French doctor, Maurice Raynaud. The literature review by Herrick and Wigley (2020) 1 is an excellent summary of all things related to Raynaud’s. There are two broad categories, primary and secondary Raynaud’s. In Primary Raynaud’s there is a defect in thermoregulation leading to an abnormal, excessive response to cold where the arteries spasm and blood flow is decreased. Interestingly, for some people the abnormal vasospasm can occur as a result of emotional stress. It typically presents between the ages of 15 to 30 years and is more common in women.
Secondary Raynaud’s occur as a complication to another disease where there is abnormal or injured blood vessels or blood vessel function. It is most commonly observed in patients with Scleroderma or other connective tissue diseases but there is a long list of diseases that can lead to Raynaud’s. It usually presents after the age of 40.
Some medications can also lead to Raynaud’s, including beta-blockers, nicotine, ergotamine, amphetamines and ADHA medication, atamoxetine and lisdexamfetamine.
Blood Flow and Thermogerulation
Blood is pumped from the heart to arteries to be distributed to cells around the body. In general, the arteries become smaller and smaller eventually ending in tiny capillaries where it connects with veins in a capillary bed. The capillary bed looks like a net surrounding the area. From there, the veins take the “old” blood back the lungs.
Smooth muscles surrounding arteries can contract to make the diameter smaller and relax to make the diameter larger. Imagine a bigger hosepipe allowing for faster and more water compared to a smaller hosepipe where the amount of water is less.
Our bodies work best when core body temperature is kept within a narrow range of 37 +/- 0.5C (98.9 +/- 0.9F). Our skin plays the biggest role in thermoregulation and we loose body heat to the external environment through radiation (60%), conduction (15%), convection (3%) and evaporation (22%) 2.
The regulation of change in diameter of the skin blood vessels play a crucial role in maintaining body temperature. In essence, warm blood flows to the skin where it loses heat to the outside, colder environment and cooled blood returns to the body.
In colder temperature, the sympathetic nervous system is activated causing the muscles contract to narrow the blood vessel diameter (called vasoconstriction). As a result less warm blood flows to skin surfaces, reducing heat loss to maintain core temperature. Following this analogy of the hosepipe, in Raynaud’s the hosepipe is suddenly squeezed closed and the water stops flowing.
Why does this happen
(This section is a bit technical, feel free to skip it.)
The cold environment (or stress activation) of the sympathetic nervous system releases noradrenaline which bind to alpha-receptors on vascular smooth muscle and the muscle contracts to narrow the blood vessels. In Primary Raynaud’s, there is a “local fault” in the blood vessels of the area (fingers). Evidence suggest there is an excessive number of alpha-2 adrenergic receptors on vascular smooth muscles. This enhances the response to the release noradrenaline and the vascular smooth muscles spasms. Repeated cold exposure further increase the number of the alpha-2c receptors again increasing the vasospasm. Not surprisingly, Raynaud’s is more common in people who live in cold climates.
When the skin is in contact with a cold object - water, ice and eve chemicals like menthol, a different subset of sensory neurons are activated. These neurons have trigger transient receptor potential channels (TRP) close to the skin surface and when triggered release neuropeptides including neuropeptide Y and CGRP. Defective TRPM8 or TRPV1 could explain the excessive vasospasms.
The cells lining blood vessels are called endothelium. Endothelial cells use the amino acid arginine to make nitric oxide (NO) with the help of an enzyme called endothelial nitric oxide synthase (eNOS). The nitric oxide diffuses into the smooth muscle cells surrounding the blood vessels to induce relaxation and increase blood flow. Defective functioning of the nitric oxide pathway has been speculated as causal in Raynaud’s.
Primary Raynaud’s could be inherited since up to 50% of patients have a close relative with the same condition. Possible culprit genes include TRPM8 and NOS1 genes
There is currently insufficient evidence for an autoimmune component for Primary Raynaud’s.
Secondary Raynaud’s manifests as an early indicator or complication of another disease or medication. Connective tissue diseases like scleroderma, rheumatoid arthritis and Sjogren’s involved damage to soft tissue - including blood vessels. As a result blood vessels do not respond normally to stimuli and are not able to restore blood flow sufficiently once temperature returns to normal.
Diagnosis
Raynaud’s is a symptom complex not a diagnosis. On presentation the first question your doctor tries to answer is “why does this patient have Raynaud’s?”. A long list of differential diagnosis needs to be evaluated. Underlying conditions needs to be ruled out since Raynaud’s can be an early sign of connective tissue diseases including scleroderma and lupus.
A doctor can confirm Raynaud’s by performing a cold-challenge - submerging hands in cold water. A microscope is used to investigate any abnormalities or damage to the capillaries under the finger nails.
Treatment
Most people with Primary Raynaud’s manage their condition with lifestyle.
It comes down to “don’t get cold”.
A good idea is to use the portable hand warmers used by skiers. Once activated, some can provide heat for 4 to 10 hours. You could also use a flexible kinesio tape to secure the handwarmer to the inside of your wrist. This will heat up the blood flowing into your hands and allow you to use your hands for everyday tasks.

Specialists in rheumatoid and related diseases may prescribe calcium channel blocker amlopidine as a first line treatment for complex Secondary Raynaud’s.
Other treatment options include phosphodiesterase type 5 inhibitors (PDE5i), endothelin-1 receptor antagonists, and statins.
There is conflicting evidence for the use of selective serotonin receptor inhibitors (SSRI) like fluexetine. Evidence is low for the use of angiotensis II receptor antagonists, alpha-blockers and oral nitrates.
The theoretical rationale for using antiplatelet agents have so far not provided good evidence. In theory, thinner blood should flow easier to help fingers and toes stay warm. Antiplatelet agents include aspirin, clopidogrel and prasugrel.
L-carnitine
A very interesting case report of two patients was published in 20033. Carnitine is an essential cofactor in the cellular energy production pathway. The patients received 330mg/d of supplemental carnitine through winter. After a few weeks they reported that their hands and feet were feeling warmer and experienced less pain. Supplementation was suspended through the warmer months and recommenced in winter.
Another study by Gasser, Matina and Dubler (1997) 4used a dose of 3g per day for 20 days. The small study of 12 patients showed that the vasospasm duration was significantly reduced and rewarming better.
Carnitine is freely available as a supplement and has no major side-effects. It is frequently added to sports supplements to increase sports performance and endurance. **
Our bodies make carnitine but we can also get small amounts from food. Food source of carnitine include beef, chicken, pork and dairy.
Arginine
A few studies5 have trialed supplementing with the amino acid L-arginine with mixed results. Blood vessel cells use L-arginine is used to make nitric oxide - a signalling molecule to relax smooth muscles and dilate blood vessels. Doses of 1-2 g/da and even up to 10g/ day has been suggested. Arginine can be purchased as a supplement over the counter.
Hopefully there will be more studies on the use of Carnitine and Arginine.
Diet and Other Nutrients
From my perspective as a clinical nutritionist, a few key foods and nutritional supplements could be helpful.
Oily fish for the Omega-3 fats. Omega-3 help keep blood vessels healthy and increase dilation. It may help to reduce inflammation from the injury caused by the vasospasm. DiGiacomo, Kremer and Shah conducted a small prospective study where 32 patients received supplemental omega-3 in the form 4g EPA and 3g DHA6. Tolerance to cold exposure was improved and onset of vasospams delayed.
Ginger as a tea increase heat and helps blood vessels dilate
Cayenne pepper contains the antioxidant capsaicin and may help blood vessels relax.
There is a case report of topical rosemary essential oil 7showing an increase in finger temperature.
**Please consult your medical practitioner before using supplements.
Support
The Raynaud’s Association is a valuable source of information.
Reference:
Herrick AL, Wigley FM. Raynaud's phenomenon. Best Pract Res Clin Rheumatol. 2020 Feb;34(1):101474. doi: 10.1016/j.berh.2019.101474. Epub 2020 Jan 29. PMID: 32007400.
Osilla EV, Marsidi JL, Shumway KR, et al. Physiology, Temperature Regulation. [Updated 2023 Jul 30]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK507838/
Rodrigues Pereira R, van Ede CM, Beemer FA. Successful carnitine therapy for Raynaud's phenomenon in velo-cardio-facial syndrome. Am J Med Genet A. 2003 Jun 1;119A(2):247-8. doi: 10.1002/ajmg.a.10490. PMID: 12749075.
Gasser P, Martina B, Dubler B. Reaction of capillary blood cell velocity in nailfold capillaries to L-carnitine in patients with vasospastic disease. Drugs Exp Clin Res. 1997;23(1):39-43. PMID: 9093821.
Curtiss P, Schwager Z, Lo Sicco K, Franks AG Jr. The clinical effects of l-arginine and asymmetric dimethylarginine: implications for treatment in secondary Raynaud's phenomenon. J Eur Acad Dermatol Venereol. 2019 Mar;33(3):497-503. doi: 10.1111/jdv.15180. Epub 2018 Aug 28. PMID: 30004597; PMCID: PMC6916181.
DiGiacomo RA, Kremer JM, Shah DM. Fish-oil dietary supplementation in patients with Raynaud's phenomenon: a double-blind, controlled, prospective study. Am J Med. 1989 Feb;86(2):158-64. doi: 10.1016/0002-9343(89)90261-1. PMID: 2536517.
von Schoen-Angerer T, Deckers B, Henes J, Helmert E, Vagedes J. Effect of topical rosemary essential oil on Raynaud phenomenon in systemic sclerosis. Complement Ther Med. 2018 Oct;40:191-194. doi: 10.1016/j.ctim.2017.10.012. Epub 2017 Nov 1. PMID: 30219447.